
Acromioclavicular AC separation Symptoms Causes Treatment Preventions & More All you need to know
AC stands for the acromioclavicular joint. AC separation is a common and frequent injury in physically active people. For example, football players or cyclists.
The clavicle or the collar bone separates from its point of attachment to the scapular or shoulder bone.
It usually happens on a fall directly in the point of attachment of the two bones. It may also happen after a direct blow to the joint, as it often occurs in contact sports.
AC separation causes functional disturbance and pain in the shoulder and arm. The injury seldom requires surgery, often resolving on its own within a week to two to three months depending upon the severity of the injury.
Return to full function is possible. The pain of AC separation is most severe when overhead movements of the affected arm are attempted.
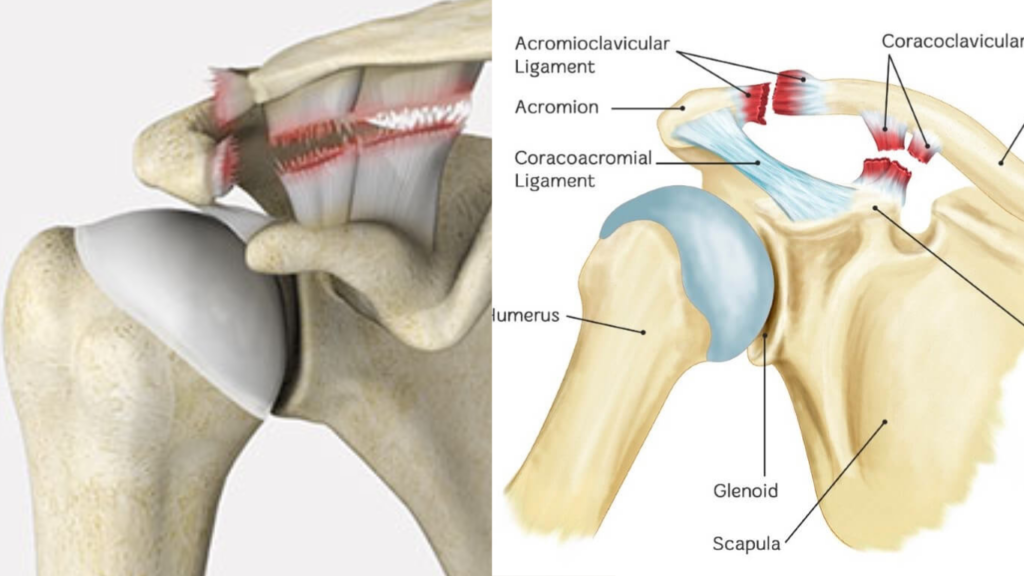
The anatomy of the acromioclavicular joint
The AC Joint is one of four joints involved in the shoulder complex. It belongs to the plain synovial joint of the gliding variety.
The joint is formed by the junction of the lateral part of the clavicle (the collar bone) and the acromion process of the scapula (the shoulder bone). The AC functions to suspend the upper limb from the trunk.
The bones involved in the AC joint are incongruent; that is, they vary in configuration. The articular surfaces may be flat-shaped, concave-convex, or reversed (reciprocally convex-concave). It varies from individual to individual.
The capsule and ligaments surrounding the joint work together to keep the bones stable. This means that the clavicle remains in contact with the acromion process of the scapula at all times.
The AC joint has a weak, thin capsule and is strengthened by ligaments both on the lower and upper sides. The attachments are further bolstered by the deltoid and trapezius muscle. Without this support, the AC joint is not stable enough to maintain its integrity.
The clavicle or the collar bone serves as an attachment for many of the muscles, including;
- Pectoralis Major (Clavicular Head)
- Sternocleidomastoid
- Deltoid
- Trapezius
Causes of AC separation
Injuries to the acromioclavicular joint are pretty standard. They account for about 40% of all shoulder injuries in contact sports. This is because of the nature of its incongruent surfaces. If the tip of the shoulder strikes a hard surface, it results in the dislocation of the joint or separation of the joint forces employed from the medial and lower side.
Any impact over the joint is resisted primarily by the joint's superior and inferior capsular ligaments. If the load or force exceeds the ability of these two ligaments, another ligament, the coracoclavicular ligament, offers a secondary resistance to horizontal shear.
Failure of these resistive mechanisms causes disruption resulting in dislocation or subluxation of the AC joint.
Some of the leading causes of AC joint separation include;
- Blow to the shoulder joint
- A fall landing directly on the shoulder or an outstretched arm
- Skiing injuries as tumbling
- Weight lifting with overhead movements
Signs and symptoms of the AC separation
The signs and symptoms vary according to the severity or grade of the AC separation.
Grade I separation
The most common type of AC injury is a slight displacement of the joint, resulting in stretching or partial tears of the ligaments.
- The joint is tender to touch
- bruising around joint
- mild pain with arm movement
Grade II separation
A partial dislocation of the AC joint in which the displacement may not be evident upon physical examination. The acromioclavicular ligament is completely torn, while the coracoclavicular ligaments are spared in this kind of injury.
- moderate to severe pain at the joint
- Swelling of the affected part
- pain with arm movement
- the top of the shoulder shows a small bump where the collar bone ends
- The clavicle may be displaced
- The area over the coracoclavicular ligaments is painful to touch
Grade III separation
Grade III is a complete separation of the AC joint. The ligaments (acromioclavicular and the coracoclavicular) are torn, including the joint capsule. There is visible displacement on physical examination.
As the support to the joint is gone, the shoulder appears to fall under the weight of the arm. The clavicle is pushed upwards and appears as a bump on the shoulder.
The typical appearance of such a patient is he/she is supporting the arm while keeping it close to the body. This position prevents any pain in the outward movement of the arm.
- Pain with movement
- The joint is painful to touch
- Swelling of the joint
- A popping sound with the movement of the joint
- Apparent shoulder deformity and a shoulder bump is seen
An AC separation may happen in six total grades. The grades mentioned above are the most common. Grade 4-6 are uncommon. They result from a high-impact and forceful injury, as in motorsports. These are treated surgically because of the severity of the injury where all the ligaments are disrupted.
The grade classification of the AC separation injury helps the physician to select the best possible therapy.
Treatment of AC separation
The treatment depends on the grade of the injury exerted on AC joint.
Grades I - III are usually treated with non-invasive methods without any operations. Such patients usually pass through a discomfort period, but the shoulder returns to full functioning after that. Some aesthetic defects may remain even after full recovery.
Some grade III injuries may require early surgical reconstruction. The decision is made on the patient's requirements. The preference of a surgeon is always to treat the injury as conservatively as possible. In worsening symptoms or progression to complications due to ill-healing, surgical reconstruction may be advised.
Depending on the grade and severity of the injury, most patients heal within 2 to 3 months without any surgery.
Return to sports is allowed upon the full and painless range of motion. The joint should not be tender to touch, and manual traction does not cause pain.
The recovery usually takes about two weeks for a grade I injury, about six weeks for a grade II and up to 12 weeks for a grade III injury.
The recommended protocol is followed as in all sports injuries.
- From the moment of impact to the first few days
- RICER
Rest the affected area and prevent any movement to reduce pain, usually with sling support for about 1-2 weeks.
- Medications
Over-the-counter analgesics and anti-inflammatory therapy are suggested.
- TENS
Since the AC separation involves ligaments and joint capsules, TENS has not an immediate role. However, after a few weeks, TENS can relieve chronic pain once any apparent injury has resolved.
- AC joint taping
Taping helps to immobilize and realign the AC joint. This is especially true in severe injures where the collar bone gets displaced upwards. The tape helps hold the bones while the ligaments and joint capsule healing.
- After few weeks or complete recovery
Patients who respond to conservative non-operative treatment return to activity in about one week for a Grade I injury to an average of twelve weeks for a Grade III injury. The following protocols should be adopted after this time.
Post-operatively, the sling is required for about four weeks. Lower arm exercises may begin immediately, but no lifting moves for three weeks.
Overhead motion is also limited for the first 8-12 weeks. This is due to the time taken by the clavicle to fix back to its attachment on the coracoid process. The recovering bones and ligaments prevent the regular rotation necessary for overhead movements.
The patient may be allowed to use the affected arm if kept at waist height to write or perform computer work for the first 12 weeks. After that time, the sutures are soft enough to endure a more aggressive range of motion and strengthening exercises.
After removing the sling, at least 6-8 weeks of physical therapy is necessary to regain full motion. However, for athletes involved in sports requiring strength and velocity, any aggressive moves may be delayed for four to six months as in throwing sports.
- Massage therapy
Massage plays a vital role in recovery and regaining the full function of the acromioclavicular joint.
Since the AC separation treatment requires a long period of inactivity and immobilization, muscle spasms are common complaints in the post-recovery phase. Sports massage and deep tissue massage help to ease away the muscle spasms.
The massage techniques used for AC separation include using deep longitudinal stripping techniques and static compression methods. The target is to treat the myofascial trigger points and muscle tightness associated with the injury.
Deep friction massage applied directly to the AC ligament is also beneficial. It stimulates collagen production in the damaged tissue. It also helps reduce scar formation by reducing excessive fibrosis during the healing process.
Massage is usually reserved for grade I and II injuries. The physiotherapist must wait until after the initial inflammatory stage (usually the first 72 hours) before administering direct friction treatment to the damaged ligaments.
Grade III and more severe injuries require a more extended period of rest before applying friction treatments. This is to ensure the avoidance of further ligament damage. It is always advised to start massage therapy consultation with the orthopedic physician who can guide accurately when massage is beneficial.
- Therapeutic ultrasound
Low-intensity therapeutic ultrasound (LITUS) works great for soft tissue recovery.
LITUS facilitates tendon healing, increasing tensile strength and improving collagen alignment. Therapeut9ic ultrasound also helps ligament injuries, as in the case of AC separation. Ultrasound increases cellular proliferation during muscle regeneration and repair.
Ultrasound therapy also speeds up healing at the tendon-bone junctions by accelerating new tissue formation. Scientific evidence backs the role of therapeutic ultrasound on soft tissue injuries encountered in AC separation and improves post-operative recovery.
- Active rehabilitation
Rehabilitative therapy must be employed to restore normal motion and to improve flexibility and strength. This should be started as soon as tolerated by the patient. Initially, gentle exercises should be employed.
Some of the rehabilitative exercises for AC separation include;
Neck rotation
- With slow and gentle movement, rotate your neck to the left, looking over your shoulder.
- Hold this position and count till twenty.
- Bring your neck to the starting position.
- Perform the same to the right side.
- Repeat at least three to four times on each side.
Shoulder rolls
- Stand tall and keep your chin slightly tucked.
- Keeping your arms relaxed, make sure to move your shoulders only.
- Move your shoulders in a shrug up toward your ears.
- Move the shoulder up and back and start making a circle.
- Circle them back and then downwards.
- Repeat at least 2 to 4 times.
Neck stretches
- Keep your arms at your shoulders' height and bring your arms forward.
- Clasp your hands in front of you.
- Drop your chin into your chest direction.
- Reach your arms straight forward and round your upper back. Hold for four to six counts.
- Repeat at least two to four times.
Shoulder blade squeeze
- Sit or stand up at your convenience with the arms at your sides.
- Keep your shoulders relaxed. They should not be in a shrugging posture but down.
- Now move your upper arm in a motion that mimics squeezing your shoulder blades.
- Hold for at least six seconds before releasing and relaxing.
- Repeat at least twelve times.
Laying down shoulder flexion
- Lie on your back with your feet comfortably flat on the floor at a convenient distance you're your body.
- Hold a wand with your hands with the palms facing down towards the floor. Hold the wand at a distance slightly wider than your shoulders.
- Keep your elbows straight.
- Slowly raise your arms overhead till a stretch is felt in the shoulders, upper back, and chest.
- Hold for a minimum of fifteen seconds before coming back to the starting position.
- Repeat at least two to four times.
- Surgical intervention
Surgery may be necessary for AC separations if they are severe enough or are non-responsive to conservative therapy for at least two to three months. Surgery can also be undertaken if there is continuous pain with movement.
Some cases of grade III injury meet the criteria for early surgery. These include;
- Young and physically active individuals (over the age of 13).
- Athletes who play contact sports
- Athletes who play non-contact sports but their physical movements are stressful and frequent
Surgery involves reconstructing the coracoclavicular ligaments and removing the distal end of the clavicle at its shoulder attachment.
Distal clavicle resection without the repair of the ligaments requires stabilization, or it may lead to excessive rotation of the scapula. Such stabilizing reconstruction techniques include;
- a fixation procedure done with pins or plates across the acromioclavicular space
- loop fixation using synthetic materials like screws and suture loops
Prevention of AC separation
Sports injuries can happen, and there is no stopping them even in the wake of adequate precautions.
Active rehabilitation is the only way to prevent recurrences. Proper warm-up before exercise and any sports activity is mandatory to prevent your body from damage.
Similarly, proper cooldown exercises to stretch the body bolsters the muscles and bones and their various attachments.

